Blank Cna Shower Sheets Form
Blank Cna Shower Sheets Form
Understanding the CNA Shower Sheets form is essential for proper skin monitoring and resident care. However, several misconceptions can lead to confusion. Here are six common misconceptions about this form:
Clearing up these misconceptions can enhance the effectiveness of skin monitoring and improve the overall care provided to residents.
Filling out the CNA Shower Sheets form is an important task that helps ensure proper skin monitoring for residents. It involves documenting any abnormalities observed during a shower. Follow these steps carefully to complete the form accurately.
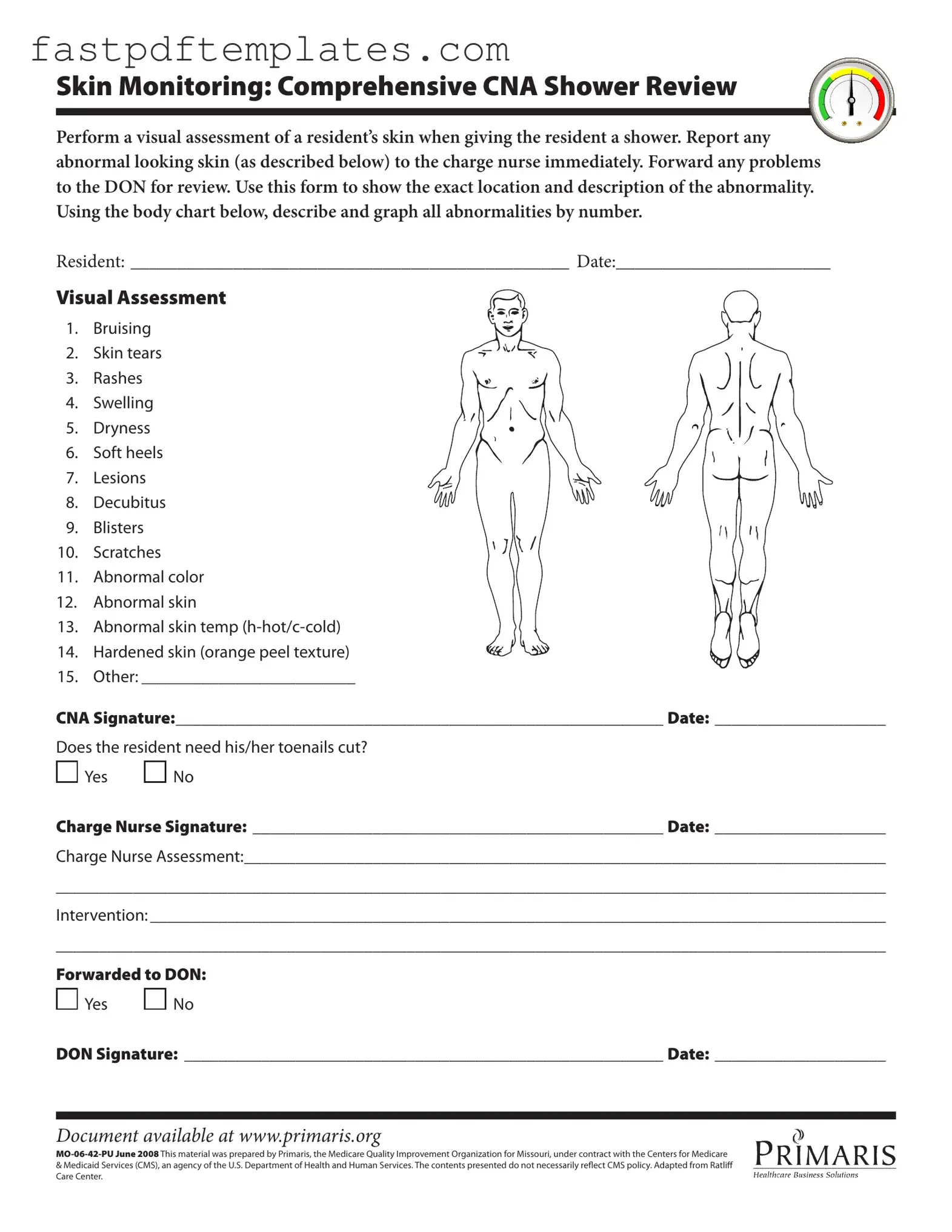
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Free Printable Direction to Pay Form - Minimize potential payment issues with your preferred repair shop.
Complemento Carta Porte - The Bill of Lading with a Supplement is a best practice in the logistics industry for international trade.
Consolation Bracket - Tournament excitement remains high throughout the bracket.
When filling out the CNA Shower Sheets form, consider the following:
Avoid these common mistakes:
Filling out and using the CNA Shower Sheets form is an important task that ensures proper skin monitoring for residents. Here are key takeaways to keep in mind:
By following these guidelines, caregivers can help maintain the health and well-being of residents effectively.
The CNA Shower Sheets form is similar to the Incident Report form. Both documents serve the purpose of documenting specific occurrences related to resident care. The Incident Report captures events such as falls, medication errors, or any other incidents that may affect a resident's health or safety. Like the CNA Shower Sheets, it requires detailed descriptions and immediate reporting to ensure that proper follow-up actions can be taken. Both forms emphasize the importance of timely communication with nursing staff and management to address any issues promptly.
Another comparable document is the Skin Assessment form. This form focuses specifically on evaluating the condition of a resident's skin. Similar to the CNA Shower Sheets, it includes a systematic approach to identifying skin abnormalities such as bruising, rashes, or lesions. Both forms require visual assessments and documentation of findings, ensuring that any changes in skin condition are tracked over time. The Skin Assessment form may also involve recommendations for treatment or further evaluation, paralleling the intervention section of the CNA Shower Sheets.
The Care Plan document shares similarities with the CNA Shower Sheets as well. Care Plans outline the specific needs and interventions for each resident, including skin care. Both documents require input from nursing staff, ensuring that assessments made during showers are integrated into the overall care strategy. The CNA Shower Sheets provide immediate observations that can influence the ongoing development of the Care Plan, making both documents essential for comprehensive resident care.
The Vital Signs Record is another document that aligns with the CNA Shower Sheets. This record tracks essential health indicators such as temperature, pulse, and blood pressure. Like the CNA Shower Sheets, it requires regular updates and monitoring to identify any changes in a resident's health status. Both forms are critical for maintaining a clear picture of a resident's overall well-being, allowing for timely interventions when necessary.
The Daily Progress Notes are also similar to the CNA Shower Sheets. These notes provide a narrative account of a resident's condition and any care provided throughout the day. Both documents require detailed observations and are used to communicate important information among the care team. The Daily Progress Notes may reference findings from the CNA Shower Sheets, creating a comprehensive record of the resident's care and any concerns that arise during daily activities.
The Medication Administration Record (MAR) is another relevant document. While the MAR focuses on the medications administered to residents, it shares the same goal of ensuring thorough documentation of care. Both forms require accuracy and attention to detail, as they are used to track interventions that impact a resident's health. Any adverse reactions noted during a shower, for example, may need to be cross-referenced with the MAR to assess potential medication side effects.
The Fall Risk Assessment form is also similar to the CNA Shower Sheets. This form evaluates the risk factors that may contribute to a resident's likelihood of falling. Both documents require careful observation and reporting of conditions that may pose a risk to residents. The findings from the CNA Shower Sheets can inform the Fall Risk Assessment, allowing for a more comprehensive understanding of a resident's vulnerabilities and the necessary precautions to take during care.
The Nutrition Assessment form is comparable as well. This document assesses a resident's dietary needs and nutritional status. Like the CNA Shower Sheets, it requires detailed observations and evaluations to identify any issues. Both forms are essential for ensuring that residents receive appropriate care tailored to their individual needs, which can include considerations for skin health and overall well-being.
Lastly, the Resident Admission Assessment form is similar to the CNA Shower Sheets. This document is completed upon a resident's admission and includes comprehensive evaluations of their health status. Both forms are crucial for establishing a baseline understanding of a resident's condition. The CNA Shower Sheets provide ongoing assessments that can highlight changes from that initial evaluation, ensuring that care remains responsive to the resident's evolving needs.
The CNA Shower Sheets form is an essential document for monitoring residents' skin health during showers. However, several other forms and documents complement this process, ensuring comprehensive care and documentation. Here’s a list of related forms that are often used alongside the CNA Shower Sheets.
These forms and documents work together to create a thorough approach to resident care. By maintaining accurate records and assessments, caregivers can ensure that residents receive the best possible support for their health and well-being.