Blank Annual Physical Examination Form
Blank Annual Physical Examination Form
Understanding the Annual Physical Examination form is crucial for ensuring a smooth medical experience. Here are seven common misconceptions that people often have:
Addressing these misconceptions can lead to better health outcomes and a more efficient healthcare experience. Be proactive and thorough when filling out your Annual Physical Examination form.
Filling out the Annual Physical Examination form is a straightforward process that requires attention to detail. Each section of the form is designed to collect essential health information that will assist healthcare providers in delivering the best possible care. Following the steps outlined below will help ensure that all necessary information is accurately recorded, minimizing the need for return visits.
After completing the form, review it for any missing information. Ensure that all sections are filled out accurately. Once verified, submit the form to your healthcare provider before your scheduled appointment.
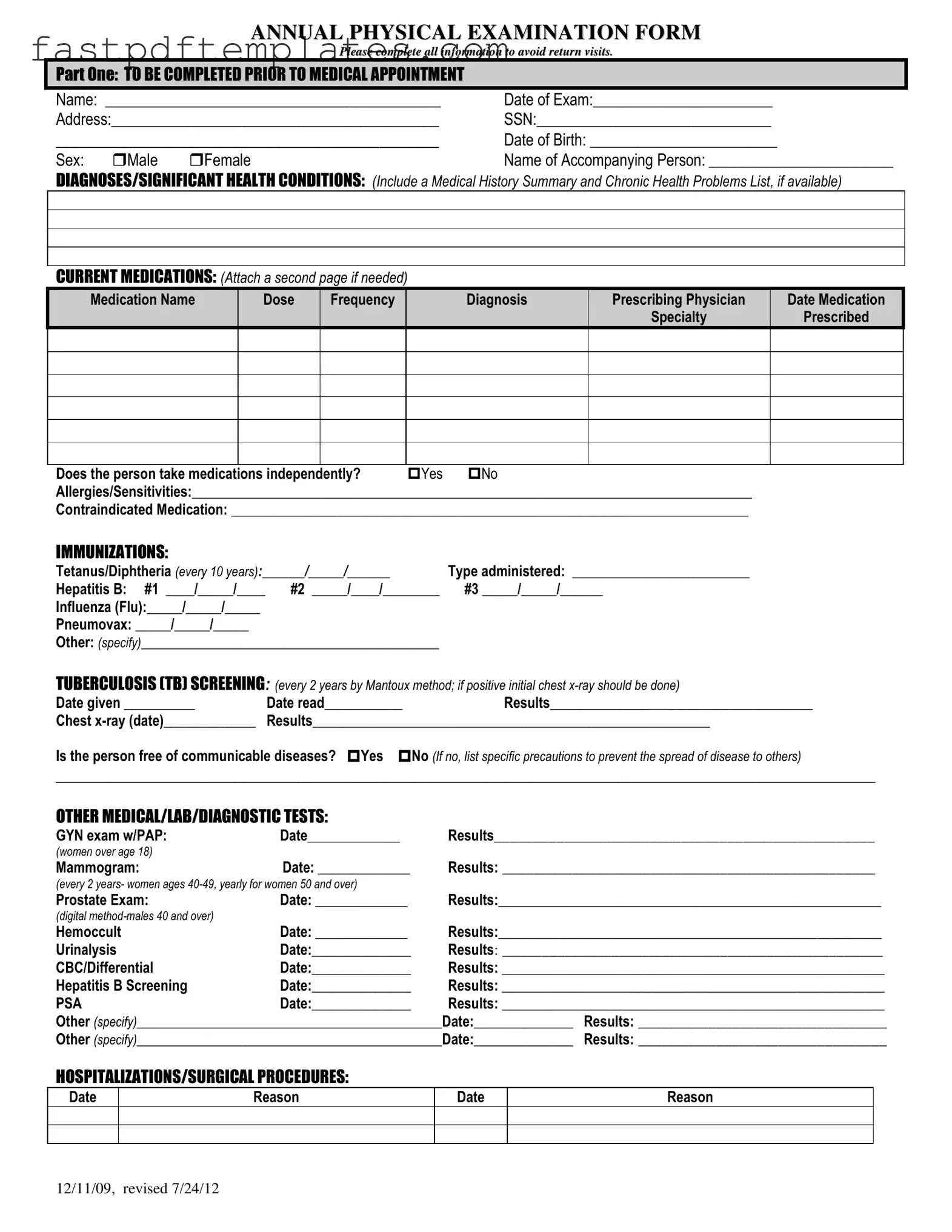
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
How to File Taxes in Florida - The Tax POA DR 835 form is a power of attorney specifically for tax matters.
What Is W9 - A proper W-9 ensures that payments made are reported accurately to the IRS.
Four Point Inspection Florida - An electrical panel photo with the interior door label is necessary for the evaluation process.
When filling out your Annual Physical Examination form, there are several important dos and don’ts to keep in mind. This will help ensure that your visit goes smoothly and all necessary information is accurately conveyed.
By following these guidelines, you can help ensure that your Annual Physical Examination is as effective and efficient as possible.
Filling out the Annual Physical Examination form can seem daunting, but it’s essential for ensuring a smooth and efficient medical appointment. Here are some key takeaways to keep in mind:
By keeping these points in mind, you can help ensure that your Annual Physical Examination goes smoothly, allowing for a more productive visit with your healthcare provider.
The Annual Physical Examination form shares similarities with the Medical History Form. Both documents collect essential personal information, including the patient's name, date of birth, and contact details. They also require a summary of the patient's medical history, which can include previous diagnoses, surgeries, and chronic conditions. This information helps healthcare providers understand the patient's background and make informed decisions about their care.
Another document that aligns closely with the Annual Physical Examination form is the Immunization Record. This record specifically tracks vaccinations received by the patient, including dates and types of immunizations. Like the physical examination form, it emphasizes the importance of maintaining up-to-date immunizations for overall health. Both documents can serve as vital references for healthcare providers when assessing a patient's health status and potential risks.
The Patient Intake Form is also similar in purpose and structure. It is typically completed before a medical appointment and gathers comprehensive information about the patient's current health status, medications, and allergies. Both forms aim to provide a thorough overview of the patient’s health, ensuring that healthcare providers have the necessary information to deliver appropriate care during the visit.
The Consent for Treatment form shares a functional relationship with the Annual Physical Examination form. While the latter assesses health, the consent form ensures that the patient agrees to the proposed medical procedures and examinations. Both documents are essential for establishing a clear understanding between the patient and healthcare provider, fostering a transparent and respectful healthcare environment.
The Follow-Up Care Plan is another document that mirrors the Annual Physical Examination form in its intent to monitor a patient’s health over time. It outlines recommendations for ongoing care, including follow-up appointments, lifestyle changes, and additional tests. Similar to the physical examination form, it aims to ensure that patients receive the necessary support to maintain or improve their health after their initial evaluation.
Lastly, the Laboratory Test Requisition form is akin to the Annual Physical Examination form in that it often accompanies a physical exam. This document requests specific lab tests based on the findings of the examination. Both forms play a crucial role in the diagnostic process, allowing healthcare providers to gather more detailed information about the patient's health and tailor their treatment plans accordingly.
The Annual Physical Examination form is an essential document that helps healthcare providers assess a patient's overall health. Alongside this form, there are several other documents that can enhance the examination process and provide a comprehensive view of a patient's health history. Here are five commonly used forms that often accompany the Annual Physical Examination form.
These forms work together with the Annual Physical Examination form to create a thorough and effective healthcare experience. They ensure that healthcare providers have all the necessary information to make informed decisions about a patient's care.